
Living with persistent dizziness, vertigo, or unsteadiness can make your world feel completely unpredictable. Simple tasks like getting out of bed, driving down the Highway 63 corridor, or checking the top shelves at a local Beaumont grocery store can become overwhelming hurdles. Many people suffering from these balance issues struggle through multiple diagnostic tests and prescription medications without finding real relief.
When structural medical imaging returns completely normal results, the underlying issue frequently stems from a functional mismatch within your inner ear balance mechanics. Vestibular rehabilitation therapy offers a highly precise, clinically proven physical pathway to reset these sensory networks and return stability to your daily life.
Decoding Your Inner Ear Balance System
What is the primary cause of chronic dizziness and vertigo? Chronic dizziness is often caused by a sensory mismatch between your inner ear’s vestibular system, your eyes, and your body’s joint sensors. When illness, injury, or displaced micro-crystals disrupt these pathways, your brain receives conflicting spatial signals, creating a false sensation of spinning or motion.
To find a lasting solution, it helps to understand how your brain tracks movement. Your internal navigation system relies on two delicate structures located deep inside your temporal bone: the semicircular canals, which track rotation, and the otolith organs (the utricle and saccule), which track gravity and forward-backward motion.
These structures utilize fluid and microscopic hair cells to convert physical head movements into constant electrical updates for your central nervous system. When working correctly, these updates coordinate seamlessly with your eyes and leg joints to keep your vision steady and your body balanced.
When an inflammation, viral infection, or physical impact disrupts this delicate network, the signals from one side of your head no longer match the signals from the other. Your eyes may tell your brain that you are sitting perfectly still, but your inner ear insists you are spinning. This internal communication breakdown causes the disorienting sensations of vertigo, nausea, and lightheadedness.
If you are experiencing these spatial conflicts, seeking out a dedicated program for Dizziness treatment physiotherapy is an exceptionally reliable way to retrain your brain to handle this sensory data correctly.
The Primary Vestibular Pathologies Treated with Physiotherapy
Which specific balance disorders respond best to physical rehabilitation? Vestibular therapy effectively treats Benign Paroxysmal Positional Vertigo (BPPV), Vestibular Neuritis, Labyrinthitis, and Persistent Postural-Perceptual Dizziness (PPPD). These non-invasive exercises clear mechanical blockages, reduce nerve hypersensitivity, and help the brain adapt to permanent inner ear deficits.
By isolating the exact mechanism behind your symptoms, clinicians can build targeted movement protocols to address your specific diagnosis.
1. Benign Paroxysmal Positional Vertigo (BPPV)
BPPV stands as the single most common cause of positional vertigo worldwide. The condition occurs when tiny calcium carbonate crystals (otoconia) break loose from their proper home in the utricle and migrate into one of the fluid-filled semicircular canals.
- The Experience: When you tilt your head back, roll over in bed, or bend down, these loose crystals slide through the fluid, creating an artificial current that triggers a brief but intense spinning sensation.
- The Solution: Because this is a mechanical problem, it cannot be cured with chemical medications. Instead, it requires precise physical head maneuvers to guide the crystals safely back where they belong.
2. Vestibular Neuritis and Labyrinthitis
These conditions involve inflammation of the vestibulocochlear nerve, usually triggered by a common viral infection.
- The Experience: The sudden drop in nerve signaling creates severe, unrelenting vertigo that can last for days, often accompanied by vomiting and, in the case of labyrinthitis, sudden hearing loss or tinnitus.
- The Solution: Once the initial inflammation passes, the nerve may be left with a permanent deficit. Physical exercises force the brain to recalibrate and adapt to the new, lower baseline signal from that ear.
3. Persistent Postural-Perceptual Dizziness (PPPD)
PPPD is a chronic functional neurological disorder that frequently develops after an acute episode of vertigo or a stressful medical event.
- The Experience: Patients describe a persistent, non-spinning dizziness, rocking sensation, or heavy brain fog that worsens in busy visual environments, like crowded shopping centers or under flickering fluorescent lights.
- The Solution: The brain has essentially become hypersensitive to motion and visual data. Therapy focuses on slowly desensitizing the nervous system to restore normal movement tolerances.
Insider Tip: The Hidden Risk of Overusing Vestibular Suppressants
Here is an essential clinical reality that many standard care guides leave out: Relying long-term on motion sickness medications actually slows down your brain’s natural ability to recover from balance problems.
When a patient experiences severe vertigo, they are frequently prescribed vestibular suppressants like meclizine, dimenhydrinate, or low-dose benzodiazepines to calm their acute nausea. While these medications are helpful for the first 48 to 72 hours of an acute attack, continuing to take them for weeks or months can become a major barrier to your long-term recovery.
These drugs function by chemically sedating your entire balance network. However, for your brain to naturally rewire itself and adapt to an inner ear issue, it needs to experience the sensory mismatch.
If you keep the system sedated, your brain never gets the clear data it needs to start the healing process. Transitioning away from chemical suppressants and moving toward an active, movement-based Physiotherapy treatment program is a necessary step to truly restore your lasting stability.
This clinical shift from chemical management to active structural habituation brings us directly to the advanced diagnostic protocols used to safely evaluate your system.
Advanced Diagnostic Mapping in Vestibular Care
How do specialists pinpoint the source of your dizziness? Clinicians map out balance issues by performing detailed physical tests, including infrared video oculography (VNG) to track involuntary eye movements, the Dix-Hallpike test for crystal detection, and dynamic posturography to measure real-world fall risks.
Diagnostic Pathway:
| Symptom Profiling ➔ Ocular VNG Tracking ➔ Dix-Hallpike Test ➔ Targeted Treatment Mapping. |
Because dizziness can stem from many different areas, a complete evaluation must look closely at how your inner ears and your eyes work together.
1. Infrared Video Oculography (VNG)
Your inner ear is hardwired directly to your eye muscles through a reflex called the Vestibulo-Ocular Reflex (VOR). This reflex is what keeps your vision perfectly steady when your head is bobbing up and down while walking.
When your inner ear is struggling, it triggers involuntary, rhythmic eye movements known as nystagmus. By placing specialized infrared goggles over your eyes in a dark room, clinicians can track these micro-movements, using the direction and speed of your eye drifts to pinpoint exactly which ear and canal are causing the trouble.
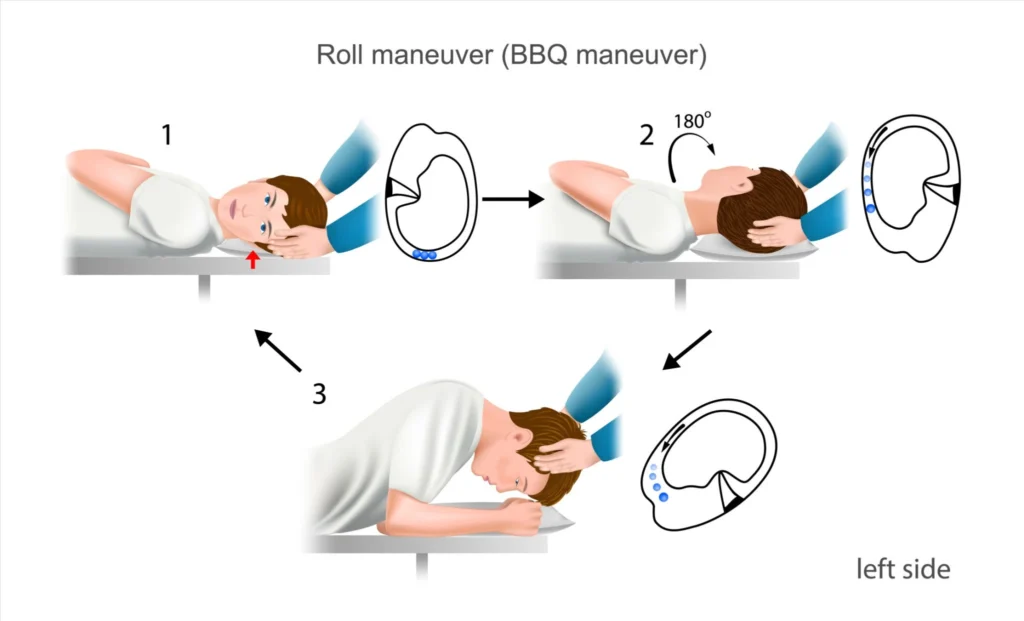
2. The Dix-Hallpike and Roll Maneuvers
To confirm a diagnosis of BPPV, clinicians guide you through specific head turns while safely lowering you into a lying position. This test alters the orientation of the semicircular canals relative to gravity. If loose crystals are present, they will slide down the canal, triggering a predictable pattern of nystagmus that tells the therapist exactly which canal needs to be cleared.
Clinical Repositioning and Habituation Workflows
What exercises are used to eliminate dizziness? Vestibular rehabilitation utilizes canalith repositioning maneuvers to clear displaced inner ear crystals, alongside gaze stabilization exercises to keep your vision clear and habituation movements to systematically desensitize your nervous system.
Once your physical diagnostic assessment is complete, your rehabilitation plan will focus on three primary therapeutic techniques:
1. Canalith Repositioning Maneuvers
If your testing confirms BPPV, your therapist will use specialized maneuvers like the Epley or Semont protocols. These procedures use sequential head tilts to harness the natural force of gravity, rolling the loose crystals through the semicircular canal and dropping them back into the utricle, where they can be naturally reabsorbed by your body. Most patients experience complete relief from BPPV within one to three sessions.
2. Gaze Stabilization Exercises
For individuals dealing with permanent nerve deficits from vestibular neuritis, the primary goal is restoring a stable visual field.
- Cawthorne-Cooksey and Adaptation Drills: Patients focus their eyes on a stationary target pinned to a wall while repeatedly shaking or nodding their head back and forth. This exercise forces the brain to compensate for diminished inner ear signals, eliminating visual blurring and bouncing when you move.
3. Habituation and Balance Training
For persistent conditions like PPPD or general age-related balance loss, treatment focuses on carefully planned exposure to challenging movements.
- Systemic Desensitization: If turning your head rapidly to the left triggers your dizziness, your program will have you repeat that exact movement at a controlled, safe speed multiple times a day. Over time, your central nervous system learns that the movement is safe, stopping its exaggerated dizziness and anxiety responses.
Essential Homeowner’s Balance Checklist
To optimize your home environment and support your recovery process, consider implementing these simple structural safety adjustments:
☑ Incorporate Pathway Lighting: Install motion-activated LED nightlights along the path from your bed to the bathroom to assist your visual balance tracking at night.
☑ Secure Loose Flooring: Secure or completely remove loose area rugs and low electrical cords to eliminate potential tripping hazards while your balance is resetting.
☑ Utilize Multi-Point Support: Add stable grab bars in your shower stall and secure handrails along all indoor and outdoor staircases.
☑ Maintain Stable Footwear: Wear supportive, flat-soled indoor shoes instead of loose slippers or walking barefoot to maximize the sensory feedback from your feet.
Frequently Asked Questions
Will vestibular physiotherapy make my dizziness worse before it gets better?
During the diagnostic evaluation and the first few treatment sessions, provoking your typical symptoms is often necessary to identify the issue and kickstart your brain’s recovery. Experienced therapists manage this process carefully, ensuring your symptoms calm down completely before you leave the clinic.
How many rehabilitation sessions are usually required to see results?
Mechanical issues like BPPV often resolve in just 1 to 3 targeted sessions. Chronic sensory matching issues, nerve injuries, or conditions like PPPD require a more comprehensive approach, typically taking 6 to 12 weeks of consistent clinic visits and daily home exercises to achieve lasting stability.
Can neck tension or cervical spine issues cause dizziness?
Yes, a condition known as cervicogenic dizziness happens when injured or tight muscles in your upper neck send faulty spatial signals to your brain. This issue frequently mimics inner ear problems and can be treated effectively by combining gentle manual therapy with targeted neck-positioning exercises.